You might think that at your Pre-op you would get a feeling for what to expect in your upcoming visit to the hospital at which your surgery will be... a feeling for the facility and the nurses and the other medical professionals that will be taking your life into their hands. What to expect when you're under the knife, and how you will be handled afterward.
I am here to tell you that that is not always how it goes - or at least I hope that is not why my day went the way it did yesterday!
I left the building with more confusion than I had when I went in, not very much confidence in the staff that looked after me, and with painful bruises on both of my cubital fossa! (hehe cubital fossa = the inside of your elbows, like, where they put in the needles to take blood - brutal vampire nurse yesterday, just sayin'!)
My Mom and I bombed down to Toronto East General Hospital yesterday to get the lay of the land for my surgery next week, and to provide health stats, bloodwork, and any information about my life that my surgeon may be missing; get all my ducks in a row for surgery. Other than the bloodwork I think it could all be done by phone or skype, or fax, or smoke signals..? But no, I had to physically trip down there to dot the i's and cross the t's.
I have done this before, I clearly remember how my pre-op was at Sunnybrook before my surgery in May, and it was no fun either - I am starting to think it may just be a symptom of pre-op visits that they are a shit-show? You don't actually get to see the surgeon, it is all looked after by nurses and pharmacists, and sometimes the anesthesiologist, though I did not see mine yesterday.
Overall, the visit did not provide a fantastic first impression of the hospital in which I will spend some time next week. Maybe I have been spoiled by the excellent care I receive at Sunnybrook, or maybe I just have a bad attitude about this thyroidectomy and node dissection(S) because I hate surgery. AND because I find it truly inconvenient that I have to have parts of my precious body removed, when really I didn't ask for this in the first place! Yes, could be a slightly bad attitude, but I digress.....
After a lengthy wait in an empty holding room (which to be fair, was nicer than Sunnybrook's pre-op hole in the wall waiting cell), I was escorted to an assessment room to have my vitals taken and my visits with various parties participating in my surgery prep.
How my blood pressure remained lower than normal through this ordeal I do not know. The nurse didn't even look at when introducing herself to me, and I find that inexcusable. I cannot imagine my paperwork being so engrossing that there wasn't time for eye contact.
Ah well anyway, after a bunch of paper shuffling and calling of other nurses to figure out just how many vials of blood I needed to give, I was very grateful that my family physician had sent extra printouts for me to take with me in case TEGH didn't receive the faxes from Sunnybrook etc. Turns out that was smart -yay Doc thanks so much for having my back! Apparently there was some miscommunication from the surgeon? Or not enough orders provided? Or..?
Two hours later, all done, bandaid on one sore cubital fossa (now please remember I get tonnes of pokes these days and I am not fussy about it, I don't watch them do it but I don't cry or wince or bitch either, but this nurse was OUCHIE) (GRRRR), jacket on and in line at the Timmies in the lobby to get a cuppa joe for the long ride home in rush hour traffic, and I hear "hellooooo hello! Hello? Look up!"
A voice in my head?? Is a deadly chandelier going to fall from the ceiling of this dump and end all my complaints about cancer in one quick crushing blow? Nope. No such luck. It was my no-eye contact vampire nurse calling from the open balcony above the lobby, asking me to please come back up - she found the paperwork and she was so glad she caught me in the lobby! grrrrr
Two more bad pokes and five more vials of blood with two more nurses involved to confer over whether or not they had the right vial colours for my apparently fancy blood test orders (does "ionized calcium" ring a bell to anyone?) that had to be contained on ice, and another 20 minutes later I was heading back downstairs to my exasperated MotherBear who had somehow contained her obvious criticism of the situation (remember, she is a retired nurse who has many times offered to do my bloodwork for me herself! LOL). We ditched the coffee run and instead broke free for the parking lot. Yes, we actually ran. As in, get us outta here!!!
Overall, not a great first impression of TEGH, and I said as much to my surgeon's assistant this morning. She apologised for the inconveniences and assured me she needed to know how things went so she can monitor their dealings with other hospitals at which her boss works. She said that I should in no way doubt my surgeon, that despite the bad first impression of the hospital, she is completely confident that I will be well taken care of next Wednesday when directly in my surgeon's hands. oh dear. I hope so!! yikes.
One of the highlights of the excitement yesterday, and the reason for my hasty call to the surgeon's office this morning, was that the nurses blithely stated that I should plan on a three day stay in the hospital - THREE DAYS IN ADDITION TO SURGERY DAY. WHAT?? I asked several times if she was sure, if that is common, if she was sure, as the surgeon told me himself that as long as everything goes okay I will be released the next day.
She said yes plan for three days and I asked repeatedly how I could find out for sure as this would be crucial information to know as I have a young family and we live three hours away!? She said she didn't know but was pretty sure - I suggested that having a backup plan in case of emergency something goes wrong is far different from PLANNING for a three day stay. Aaaarrrghhhhh
Long story short, this morning my surgeons office confirmed that I need only plan for one nights stay, unless there should be an emergency. They used to keep people in intensive care for three days after a thyroidectomy, due to necessary monitoring of calcium levels, but not anymore. So... as it stands, I am expecting to come home Thursday Dec. 4.
Lots of shuffling has happened since I got the surgery date, but we are now one week out and I think it is all organised. Scott will be taking me to my operation, we will be in Toronto Tues. Dec. 2 through Thurs, Dec 4, and my Mom is coming to stay with the girls and taxi them to and from school, ankle x-rays, and play performances etc. Then Scott leaves for work likely on the Friday, Mom will stay until Sunday, and Grandma Iris is coming first of the following week to help taxi and look after the girls while I rest and recuperate for a few more days. Yes, I do expect to get some much-needed rest in my cozy master suite LOL - can I start now?? ;-)
No confirmation of post-operative assessment date, but looks like it will be one week after surgery, on or about Dec. 11, 2014.
In any case, I suppose I am grateful that the pre-op is over with and an accomplishment to add to my cancerous list, but I am grateful that my post-op care will continue at Sunnybrook and the whole thing will be behind me about a week from now. I will be tired I am told, and I will have to start taking a supplement to replace my natural thyroid function, and I will have to start taking a calcium supplement, but otherwise everything is rolling along as it should.
I am just about to the point where there is nothing else I can do to prepare for this thing, so I have to let it all go and just roll with it. I lost control of this bus ages ago!!
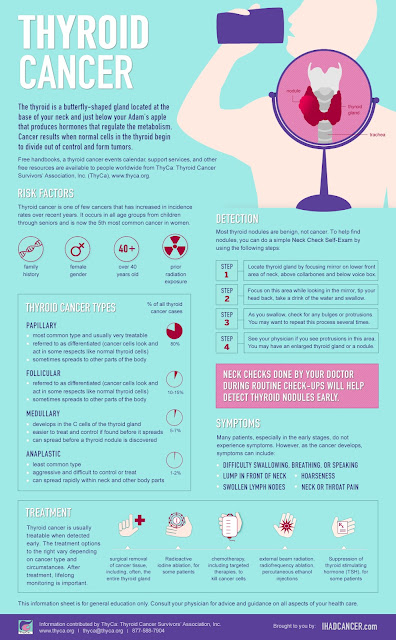
I'm not supposed to look this stuff up, but if you want to know more about my diagnosis of Papillary Thyroid Cancer, this is where I would maybe start looking. Here too. :-) Oh and Canadian site here: http://www.thyroidcancercanada.org/
Thyroid Hormone Replacement and Papillary Thyroid Cancer?
Regardless of whether a patient has just one thyroid lobe and the isthmus removed, or the entire thyroid gland removed, most experts agree they should be placed on thyroid hormone replacement for the rest of their lives.
This replaces the hormone in those who have no thyroid left, and
to suppress further growth of the gland in those with some tissue
left in the neck.
There is good evidence that papillary carcinoma
responds to TSH secreted by the pituitary, therefore, exogenous thyroid
hormone is given, which results in decreased TSH levels and a
lower impetus for any remaining cancer cells to grow. Recurrence
and mortality rates have been shown to be lower in patients receiving
suppression.